a. It is my will and strong conviction of conscience that all women and men are endowed with natural rights (aka fundamental rights, God-given rights, unalienable rights) — in the case of vaccines, the simplest way of putting it is, “my body, my choice.”
b. Natural rights are enshrined in numerous internationally recognised legal codes. With specific reference to medical treatments, especially those which are experimental; it is clearly established by the Nuremberg Code that no one should be forced or coerced in any way to have medical treatments.
c. It is my will and strong conviction of conscience that a healthy and active immune system in most circumstances does the best job of protecting one’s health from microbe-pathogens that may cause disease in humans.
d. Injecting foreign substances into one’s body is unnatural and an act the will cause a synthetic response of one’s immune system. During this response one’s immune system will either; have a positive reaction or a negative reaction. The extent of each reaction varies. No matter what the level of the safety and efficacy of an inoculation, there is always a risk for some recipients to be affected by adverse events. To justify taking the risk of suffering an adverse event one must conduct a personal risk/benefit analysis. To determine a course of action one needs to have at their disposal as much information/evidence of the pros and cons as one can discover (*Please note: pertinent undisclosed or discovered evidence can influence the decision.) The preponderance of evidence, together with a rational, logical thought process, based upon one’s will and conscience is what will govern one’s personal choice.
Related to SARS-CoV-2/COVID-19 (CV19) specifically:
1. The projected population infection rates were grossly overstated. At present, as bad as it is in the UK, the infection rate is no more than 8.6% of the total population (with lockdowns & 1900 deaths per million). Contrast this with Sweden, which had an infection rate of 10.8% (no lockdowns & 1438 deaths per million). Belgium had a population infection rate of 9.66% (with lockdowns & 2168 deaths per million) Australia’s population infection rate is 0.48% (with lockdowns & 54 deaths per million).
2. The lethality of CV19 has been grossly exaggerated. “Most locations probably have an [overall] infection fatality rate[1] less than 0.20%”[2] which is significantly smaller (at least 20 times less) than the initial projections by the authorities of an infection fatality rate of 4.0% (W.H.O.).
3. The data shows that CV19 may be a tiny bit more hazardous than the flu for some people (under 70 years) and much less for others (under 30 years).
4. There is no hard-scientific evidence that CV19 asymptomatic transmission exists, let alone that asymptomatic transmission is a driver for the CV19 ‘pandemic.’ *Please note: the perception of asymptomatic transmission existence is however, a significant driver for the lockdowns. And lockdowns have been shown by numerous studies to be only marginally effective in the control of CV19 cases. While lockdowns seriously disrupt the nation interest (economic-health), destroy medium/small businesses and causes a ‘devastating’ effect on human mental health i.e. increased suicide.
5. Besides the inoculations there are other drugs (off-label/re-purposed), used in unison, that provide a significant reduction in CV19 symptoms. i.e. Ivermectin (But worse, they have been suppressed by the TGA) *Please note, recent clinical studies have concluded these drugs are safe and effective.
6. The same off-label/re-purposed drugs from item 5 have also shown to provide prophylactic protections as well. i.e. Ivermectin (And also suppressed by the TGA)
7. Even without treatment an individual between 50 - 70 years of age who contract the illness has a 99.5% chance of recovery.
8. Those older than 70 years of age without treatment have a faction lower than 99.5% chance of surviving.
9. Younger peoples’ chances of surviving without treatment are excellent, higher than 99.99%.
10. The number of cases is grossly exaggerated by the inadequate and not suited to purpose diagnostic tool i.e. rPT-PCR testing.
11. The testing of healthy individuals and the poor test methods exaggerate the ‘cases.’ Testing over reach *Please note: the reason for testing healthy people; is the belief in asymptomatic spreaders, this is ridiculous.
12. The virus has not been purified, therefore not properly identified for gene-sequencing.
13. The gene-sequencing code used to diagnose the illness is not based on reality but an ‘in silico’ (computer) construction model. A test result returning a positive becomes a ‘case’ but in fact that ‘case’ may not be infected at all, but is still counted as a CV19 case.
14. In addition, if you haven’t got the real gene code of an illness, how is it even possible to create a safe and effective inoculation to combat it?
15. The CV19 shots are experimental and are in ‘trial use,’ were rushed into usage under the mis-perception there was a medical emergency i.e. SARS-CoV-2 pandemic, yet under any reasonable measure i.e. items 1 through 14, the medical emergency is bogus.
16. There is no medical emergency requiring emergency use of experimental treatments. Off-label/re-purposed drugs are proven to be effective and much safer than unproven experimental inoculations!
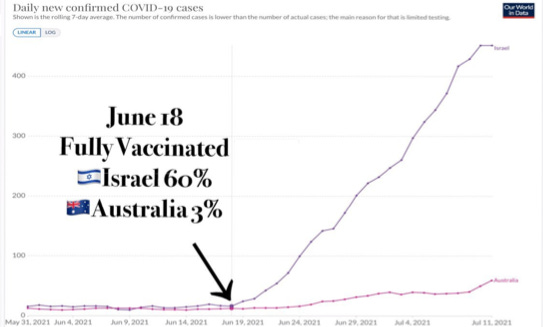
17. According to the pharmaceutical companies the inoculations do not prevent infection but limit the symptoms. It has been reported from Israel that the Pfizer jab has reduced its effectiveness and this is why an additional booster is being discussed. *Please note: if the jabs don’t prevent infection, what’s the reason for the ‘vaccine-passport’?
18. Also, the inoculations do not prevent transmission. As can be seen CLEARLY from the reports from Iceland and Israel. (So, what’s the reason for the vaccine-passport? This is also a Human Rights infringement)
19. There is no way to know the long-term health effects of these shots (which technically, are not vaccines but gene-therapy) because they were rushed into use before proper studies were done or completed.
20. The synthetic spike protein produced by the injections are cytotoxic (toxic to living cells) and does not stay in the location as expected but quickly disperse throughout the body. In women these spike proteins congregate in the ovaries, raising concerns about reproductive issues.
21. The available adverse event data clearly shows the inoculations are not safe, by any previous measure, i.e. 50 years of Australian vaccine safety data. (see Appendix B)
22. Cytotoxic nature of the inoculations has the potential to cause untold number of serious short and long-term damage to peoples’ bodies (including death!).
23. There are indications that the inoculations are becoming antibody dependant enhanced (ADE).[3] (see Appendix C)
24. The government cannot alone be trusted to advise individuals about personal health decisions. There’s a significant difference between making decisions for a population and one’s personal circumstances.
25. Removing the safety and efficacy checks and balances from new vaccines is unacceptable. No profit driven company (i.e. Pharmaceuticals) should be trusted to self-regulate the production of medicines when huge profits are at stake,especially those that are regularly fined billions of dollars for promoting ineffective, dangerous and unnecessary medications. Profits above health.
26. Never before has the onus been placed on scientists outside the vaccine companies to prove danger. It has always been the responsibility of the companies to prove safety and a lack of data regarding harm does not equal confirmation of safety.
27. Recent evidence has surfaced that available published papers strongly suggest the SARS-CoV-2 is a chimeric (Gain-of-Function) coronavirus.[4]This means the genetic code is synthetic and by definition is a bioweapon.
28. Given item 27, the inoculations are the result of a synthetic genetic code and aretherefore a bioweapon by-product.
29. RT-PCR (Real Time-Polymerase Chain Reaction) tests are not an appropriate diagnostic tool and with high cycle rates returns very high numbers of false-positive results. The PCR test can detect almost anything microbial, no matter how tiny, but it cannot determine how much of the microbe is there. PCR tests detect viral fragments from nasal or throat samples using cycle thresholds (amplification). If viral fragments are found at lower thresholds (1-30), that indicates a lot of the virus is likely present because it was found quickly. But if cycle thresholds cycle beyond 30 times,[5] it means the viral fragments are so few that they are impossible to detect. Instead, a microbial piece of dead virus or nucleotide is detected and easily mistaken for the virus fragment. Precisely because PCR tests are purely qualitative (and not quantitative), this molecular testing technology heretofore has been universally rejected as preliminary diagnostic tools for infection and disease. Predictably, as a result of PCR's predominate use in diagnosing COVID-19, increasing numbers of medical and science professionals are uneasy because 70-90 percent of positive PCR test results, generated using 35 or higher cycle thresholds, are “false positives,” requiring additional testing for definitive case confirmations.
30. The inoculations use foetal cell-lines during the manufacturing process. For people of religious faith (i.e. many Christians, including me), this is a serious moral impediment to accepting the inoculation.
31. There are available a number of safe and effective off-label/re-purposed drugs that provide a reduction in symptoms and also provide prophylactic protection is a comforting factor. There are also a large number of early-treatment protocols which are proven to be very effect.
32. My conclusion is: the fundamental rights, moral considerations (conscientious objection), together with balancing the personal risk/benefit of the experimental gene treatment (which carries with it conceivable/possible serious known and unknown medical complications, which includes death) there is in my view the experimental gene treatment poses a far greater threat to my short, medium and long-term health than the possibility of contracting and dying from COVID-19. Put simply, the CV19 inoculations concern me more than contracting Covid-19
Sound advice from an expert - Robert Malone
The inventor of mRNA vaccines and RNA transfection, Dr. Malone has extensive research and development experience in the areas of pre-clinical discovery research, clinical trials, vaccines, gene therapy, bio-defense, and immunology. He has over twenty years of management and leadership experience in academia, pharmaceutical and biotechnology industries, as well as in governmental and non-governmental organizations.
Dr. Malone is a specialist in clinical research, medical affairs, regulatory affairs, project management, proposal management (large grants and contracts), vaccines and biodefense. This includes writing, developing, reviewing and managing vaccine, bio-threat and biologics clinical trials and clinical development strategies. He has been involved in developing, designing, and providing oversight of approximately forty phase 1 clinical trials and twenty phase 2 clinical trials, as well as five phase 3 clinical trials. He has served as medical director/medical monitor on approximately forty phase 1 clinical trials, and on twenty phase 2 clinical trials, including those run at vaccine-focused Clinical Research Organizations.
Scientifically trained at UC Davis, UC San Diego, and at the Salk Institute Molecular Biology and Virology laboratories, Dr. Malone is an internationally recognized scientist (virology, immunology, molecular biology) and is known as one of the original inventors of mRNA vaccination and DNA Vaccination. His discoveries in mRNA non-viral delivery systems are considered the key to the current COVID-19 vaccine strategies. Dr. Malone holds numerous fundamental domestic and foreign patents in the fields of gene delivery, delivery formulations, DNA vaccines and mRNA vaccines.
He received his medical training at North-western University (MD) and Harvard University (Clinical Research Post Graduate) medical school, and in Pathology at UC Davis.
Dr. Malone has close to 100 peer-reviewed publications and published abstracts and has over 11,477 citations of his peer reviewed publications, as verified by Google Scholar. His google scholar ranking is “outstanding” for impact factors. He has been an invited speaker at over 50 conferences, has chaired numerous conferences and he has sat on or served as chairperson on numerous NIAID and DoD study sections.
Dr. Malone’s positions relating to COVID Vaccines
1) Bioethics require full risk disclosure and free choice. Neither of these are being met.
2) For high risk populations, the risk/benefit ratio for the USA vaccines seem to make sense.
3) We do not know all the risks yet.
4) For paediatric and young adult populations, the data does not currently support adequate risk/benefit for USA vaccines. So, stop!
7) Attacking others credibility as a way to win arguments is the refuge of the stupid.
8) Dr. Geert Vanden Bossche[7] is completely correct as a virologist and vaccinologist in everything that I have read of his. Time will prove him right - I am confident in that. But IMO (in my opinion) as a physician, the death and disability in the high-risk populations still merits vaccination.
9) There is a concerted effort to suppress information [refer item 1] and dissent in support of the noble lie.
10) The noble lie is-
a) We have to reach herd immunity for economic recovery and to minimize death and disability,
b) These genetic vaccines are the only path available to herd immunity,
c) These genetic vaccines are perfectly safe.
Each of these statements are demonstrably false.
Appendix A
Australia Total Tests 25,181,921 (Approx. cost $5 Billion)
Resulting in 34,384 ‘cases’ = Test Infection Rate (unadjusted)
It took 50 years on the TGA Adverse Events reporting to come up with 59 Coincidental Deaths from Vaccines (Properly approved Vaccines) It took 5 months on the TGA Adverse Events reporting to come up with 564 Coincidental Deaths from Experimental Covid19 Vaccines (Provisionally approved Vaccines)
And the TGA has stares this in the face; insulting the dead family members that reported these events by stating about 1 percent of them can be "confirmed" as being caused by the Vaccines.
It is a growing common knowledge that hospitals and Doctors are brushing off side effects and failing to report side effects; even deaths that are clearly "coincidental" to the TGA's adverse reaction system. As such these Doctors and Hospitals become increasing liable for the deaths and injuries of those that take the vaccines, that would not have taken them but for the cover up or malfeasance of the Doctors that decide not to report the "coincidence".
From a study of mature VAERS Data (to the end of January 2021 - where the TGA has caught up with the reports) There were 2754 "reported" Deaths after 49.22 Million Experimental Vaccine Doses. This equates to the need to "report" a death every 8936 full vaccinations
Don't be fooled by double talk from Health Authorities that use language like "confirmed" deaths; the relative danger of these vaccines cannot be argued away with deceptive words; to do so is to make a mockery of the reporting system and its 50 years' worth of records.
John Skerrit is responsible for the TGA and directly responsible for the provisional approval of these experimental vaccines.
He is fully aware of the emerging dangers of these vaccines and now the failed efficacy of the vaccines as is clear from Israeli, UK, Iceland and US Data. Further he is fully aware of early treatment protocols that Doctors around the world are using and reporting major success.
Worse still, John Skerrit is responsible for the continued scheduling decision of his TGA to classify
Hydroxychloroquine as a Poison (after 50 years of extra-ordinary safe use; it becomes a poison - some say to make way for a Vaccine only solution); taking away his fellow Australian's treatment options and funnelling them into an uninformed and coerced consent of novel technology experimental vaccines.
Vaccines with gaping holes in short term safety; having never been tested on Children, the Elderly, Pregnant or the Immune Compromised yet pushed/recommended onto them all by the TGA.
Vaccines with NO medium-term safety data; we have no idea what the circulating spike
proteins will do to the Ovaries, the Testes the Brain and other areas and organs of the body where it is now known that the spike proteins circulate and concentrate for a number of weeks.
We have no Safety Data for the Long-term effects - foetal development - future fertility - Primed Immune Response - NONE have been ruled out with ANY safety data.
With Clive Palmer about to take Prime Minister Scott Morrison to court; it looks like it is could be on
the cards for Negligent Manslaughter charges to be levelled at the TGA's front man - John Skerritt for letting things continue for so long presumably to satisfy the proponents of a Vaccine led magic bullet to let everyone out of their intermittent cages.
Anyone doubting the Video and how the table was created here are the urls as used in order:
As of August 2021 - the seemingly State-Run Media is still refusing to allow ANY discussion of early covid19 treatments saving lives around the world.
The National Covid19 Clinical Evidence Task force headed by Associate Professor Julian Elliott has failed to do anything but make negative recommendations and fuel fear inthe Australian Community
Their failure to recognise even the slightest possibility that the thousands of Doctors around the world successfully using Early Treatments might have something to offer Australia is negligent in the eyes of many; perhaps negligent manslaughter worthy.
Here's what they could easily have recommended if they were not committed to Experimental Vaccines and towing the line of vaccine proponents:
Please download it - show it to your doctor as your doctor why hasn't he got a plan like this; is it because there's no supporting evidence.....
https://hcqmeta.com/
https://ivmmeta.com/
Some idiots will refuse to look at the papers on it and say "who wrote these web pages up"
Simple answer - the thousands of authors involved in the hundreds of peer reviewed papers that it references, papers that anyone can find themselves if they want to do the legwork ; perhaps on Pubmed...
Try these links
http://tribeqr.com/v/pubmedhcq
http://tribeqr.com/v/pubmedivermectin
Would these discerning early treatment skeptics also want to question the web developers of Pubmed?
When will more people wake up to the corruption that is the Mainstream Media working with Vaccine Proponents all in unison to push the jabs even deeper into the Experimental public and to create vaccine "believers" - so many people already have seen through the "state run" Media...
Appendix C
Iceland has the world’s 3rd highest % of their population vaccinated against COVID.
They currently have more covid cases than they have ever had.
So, over two years later the assessment can be made. Did I get it right?
YOU’RE DAMNED RIGHT I DID!
[1]infection fatality rate, means the proportion of people who die from a specified disease among all individuals diagnosed with the disease. f
[2] John P A Ioannidis, Infection fatality rate of COVID-19 inferred from seroprevalence data, Meta-Research Innovation Center at Stanford (METRICS), Stanford University. This is a Bulletin of the World Health Organization, 99 (1), 19 - 33F. World Health
Thanks for reading Gaz’s Substack! Subscribe for free to receive new posts and support my work.
[3]Antibody Dependent Enhancement (ADE), occurs when the antibodies generated during an immune response recognize and bind to a pathogen, but they are unable to prevent infection. Instead, these antibodies act as a “Trojan horse,” allowing the pathogen to get into cells and exacerbate the immune response. The simple definition of ADE is “raising antibodies that don’t protect, but actually make a viral infection even worse”.
[4] Dr. Richard M. Fleming, Is COVID-19 a Bioweapon? A Scientific and Forensic Investigation, Skyhouse Publishing, 2021.
[5] NSW Pathology report on their website that ‘Generally, the number of cycles run by the PCR systems is 45, however this can vary depending on the machine or assay used. Generally the cut-off or threshold is set at a Ct of 40.’ https://www.pathology.health.nsw.gov.au/covid-19-info/sars-cov2-nat
[6] “Freedom of expression is the foundation of human rights, the root of human nature and the mother of truth. Killing freedom of expression is insulting human rights, it is repressing human nature and suppressing the truth. Liu Xiaobo ”. Defender of human rights and Nobel Peace Prize in 2010.
[7] Vanden Bossche’s scientific argument in broad terms is that the current COVID-19 vaccines, through a mechanism analogous to antibiotic resistance, will create mutant variants of the virus that escape the protection of those vaccines. This problem will be exacerbated, he claims, because people who have been vaccinated (and/or social distancing and staying inside during the pandemic) will be less capable of fighting off those strains than someone who has not been vaccinated.









Great post! Thank you!
The World Health Organization has clearly violated the International Health Regulations and they are actively conspiring to violate them again.
Take action to make sure that your Senators, Representatives and Members of Parliament are aware of these violations by the World Health Organization.
how to stop the rot from the top https://jamesroguski.substack.com/p/dear-senator